Neuro Oncol. 2012 Oct 25. [Epub ahead of print]
A phase I/II trial of vandetanib for patients with recurrent malignant glioma.
Kreisl TN, McNeill KA, Sul J, Iwamoto FM, Shih J, Fine HA.
Source
Neuro-Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, Maryland (T.K., K.M., F.I., J.S., H.F.); Biometric Research Branch, Division of Cancer Treatment and Diagnosis, National Cancer Institute, Bethesda, Maryland (J.S.).
Abstract
Vandetanib is a once-daily multitargeted tyrosine kinase inhibitor of vascular endothelial growth factor receptor-2, epidermal growth factor receptor, and the rearranged-during-transfection oncogene. A phase I trial was conducted to describe the pharmacokinetics of vandetanib in patients with recurrent glioma on enzyme-inducing anti-epileptic drugs (EIAEDs) and to identify the maximum tolerated dose (MTD) in this population. A phase II trial evaluated the efficacy of vandetanib in patients with recurrent malignant glioma not on EIAEDs as measured by 6-month progression-free survival (PFS6). In the phase I trial, 15 patients were treated with vandetanib at doses of 300, 400, and 500 mg/day, in a standard dose-escalation design. The MTD in patients on EIAEDs was 400 mg/day, and steady-state levels were similar to those measured in patients not on EIAEDs. Dose-limiting toxicities were prolonged QTc and thromboembolism. Thirty-two patients with recurrent glioblastoma multiforme (GBM) and 32 patients with recurrent anaplastic gliomas (AGs) were treated in the phase II trial, at a dosage of 300 mg/day on 28-day cycles. Six patients (4 GBM, 2 AG) had radiographic response. PFS6 was 6.5% in the GBM arm and 7.0% in the AG arm. Median overall survival was 6.3 months in the GBM arm and 7.6 months in the AG arm. Seizures were an unexpected toxicity of therapy. Vandetanib did not have significant activity in unselected patients with recurrent malignant glioma.
|
 肺癌术后2年重获新生,不焦虑不内耗
讲述者:黄宇星整理者:pear编者按“用实力坚持到胜利”ALK阳性非小细胞肺癌患者摄影
肺癌术后2年重获新生,不焦虑不内耗
讲述者:黄宇星整理者:pear编者按“用实力坚持到胜利”ALK阳性非小细胞肺癌患者摄影
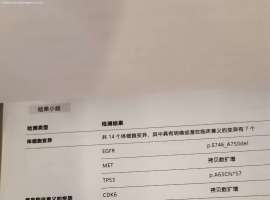
 基因检测结果刚出来,麻烦懂得病友帮
我母亲刚确诊是肺腺癌晚期,基因检测结果刚出来,麻烦懂的病友帮忙给看一下
基因检测结果刚出来,麻烦懂得病友帮
我母亲刚确诊是肺腺癌晚期,基因检测结果刚出来,麻烦懂的病友帮忙给看一下
 肺癌精准诊疗再“升级”:首部《EG
作者:雨过天晴
肺癌治疗已进入“精准时代”,靶向药物让许多EGFR突变患者获得了更长
肺癌精准诊疗再“升级”:首部《EG
作者:雨过天晴
肺癌治疗已进入“精准时代”,靶向药物让许多EGFR突变患者获得了更长
 史美祺教授、李咏生教授:MET扩增精
整理者:雨过天晴审核人:鹰版为帮助MET基因异常等少见靶点NSCLC患者解决在治疗过程中
史美祺教授、李咏生教授:MET扩增精
整理者:雨过天晴审核人:鹰版为帮助MET基因异常等少见靶点NSCLC患者解决在治疗过程中
 10个月伏美和谷美耐药了,求助新方案
母亲 55岁 161 53kg 低分化腺癌晚期
查出来的时候脑转 骨转 肝转
24年11月底基因检
10个月伏美和谷美耐药了,求助新方案
母亲 55岁 161 53kg 低分化腺癌晚期
查出来的时候脑转 骨转 肝转
24年11月底基因检






 显身卡
显身卡



